"To the appropriate RAH medical professionals re Pam Fiesley’s dislodged PEG tube,
When Pam came home some days after the insertion of her new Jejunum PEG tube, I found the tube ridiculously long as it was getting caught regularly, because of its length, around Pam’s abdomen and elsewhere during the normal manipulations of her, needed for her washing, dressing and lifter-sling implementations.
I eventually cut it to a reasonable length by removing 51cm
off its original length, but did so only when I had determined that it was just
a simple tube – not a tube within a tube as was the former stomach PEG.
Given that the previous tube allowed for a position-locking
water-filled balloon as well as a separate feeding tube, it had me wondering
how this new Jejunum PEG was being locked in place. I did notice that originally a single stitch
into Pam’s abdomen was apparently holding it in place, but it was only a day or
so after that, that the attachment failed.
It wasn’t too many days later still that I noticed that that very suture
thread wrapped around the tube was now about 1cm away from Pam’s skin – ie 1cm
of the PEG tube had come out.
Pam’s wound site was being daily dressed by a visiting nurse
and I asked her if she could please determine for me how this PEG tube was supposedly
fixed in place, as it didn’t really seem to be.
Nevertheless, it still functioned as it should and the 1cm of exposed
tube didn’t appear to get any worse. Unfortunately the
nurse didn’t get back to me re that inquiry.
This morning, when I disconnected Pam’s PEG feed equipment,
the newish (3-week old) PEG tube seemed as it had for many days – unsurprising;
but by the time I had Pam washed, dressed, lifted and transported to her lounge
chair, the PEG tube had completely dislodged and I only noticed this when I
reached under Pam’s nighty to find and expose the PEG nozzle ready for Pam’s
9:00am medication and hydration flush. I
found instead, that I had the entire tube in my hand.
At least I could now see at once what had been holding this
tube in place – nothing whatsoever! When
I think about it, it surprises me that it actually stayed in place for the 3
weeks and 2 days.
Pam is extremely frail and the anaesthetic required for the initial
insertion of her PEG tube was highly dangerous and life-threatening as it was then
explained to me, so with respect, wouldn’t it have been reasonable to ensure
that the tube was securely and permanently positioned, first time around?
I now politely beg you to use a new PEG tube with a better
designed securing method.
Yours sincerely,
Eric Fiesley."
I gave it to Pam an hour ago to take to Adelaide as she is getting air-ambulanced back there to have another PEG tube fitted. Since writing that letter however, I have been giving thought as to what purpose that absurd length of PEG tube might have been used for, given I have now found out, the hard way, that there was nothing holding the tube in place. I reasoned that the extra length could have perhaps been coiled and stuck to Pam’s abdomen with tape, leaving just a reasonable length for normal use. This coil would certainly protect the entry point from the traumas that the nozzle-end gets in day-to-day use
However, when I took Pam back
into my care, there was no coil – just ¾ of a meter of narrow rubber tube which
(as I mentioned in the above letter) would get wrapped around Pam, her pillows,
her leg – you name it – and regularly pull at the entry point. I figured
that there must be some sort of locking mechanism in place and that this
‘catching’ was needlessly testing it out and so I shortened it. Nobody
had explained why it was so long and, more importantly, that there was
absolutely no locking mechanism in place. Given the latter information, I
might have reasoned that the additional length was for coil-buffering. I
dare say, I’ll find out in the next day or so if they choose to realise at last
that proper communication is a good idea.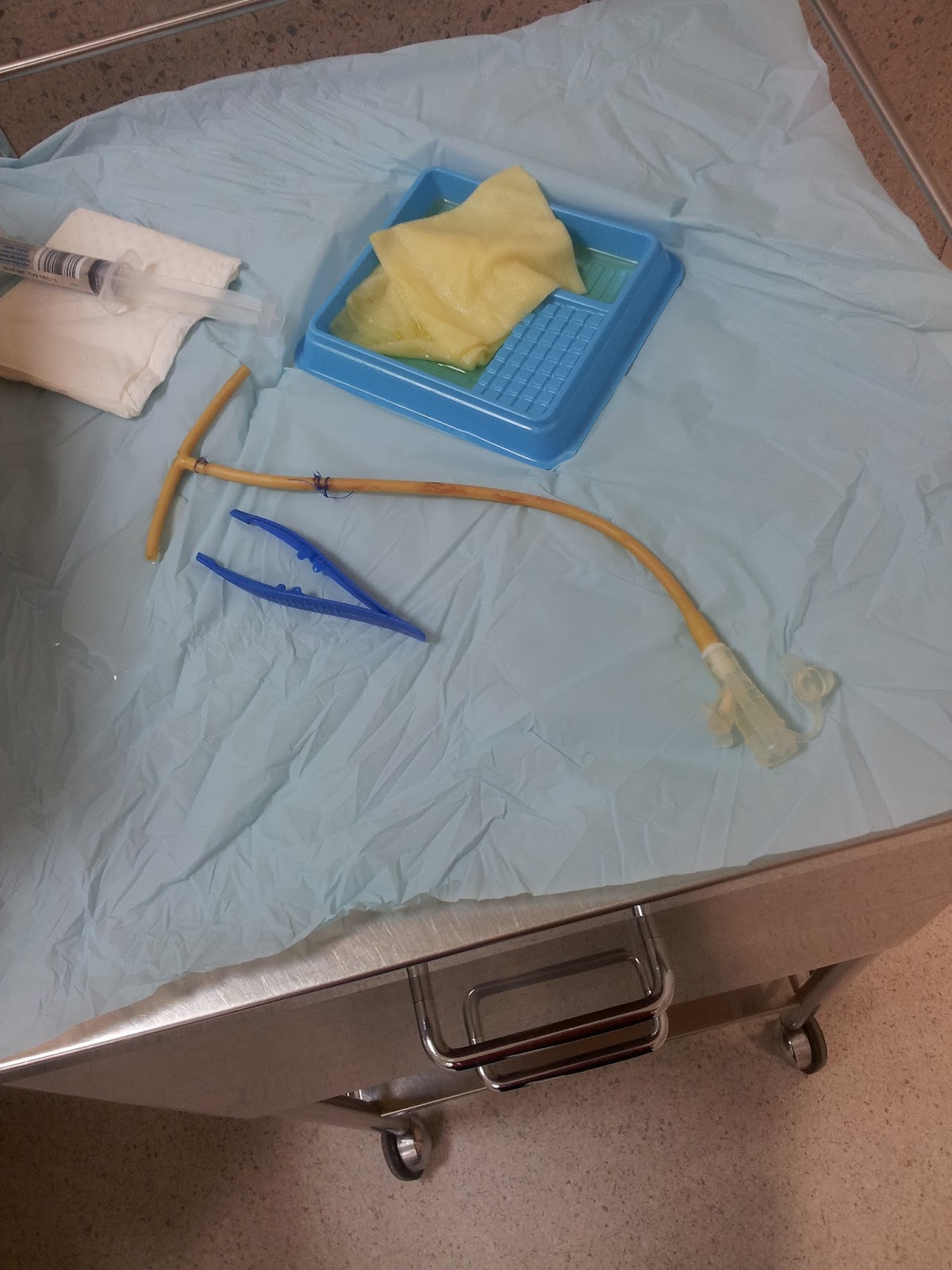
Here is a picture of the PEG tube that came away. It was sitting on a Mildura Base Hospital bench when I took the picture (they wanted to keep it, for some reason). It would seem at first site that the 'T" piece which would have been in Pam's jejunum, would have been ample as a locking device, but sadly it’s nothing of the sort.
It’s made of the same soft rubber as the rest of the PEG tube, and has also been split completely along its length to allow an even distribution of the feed. This slit however, makes it even more flimsy and entirely useless as a locking device. Remember, the tube used to be 51cm (duh, that’s over ½ a metre) longer – and maybe I should have left it so. Who knows? As I said above, I dare say I'll soon find out!
A couple of days have come and gone, and there's quite a bit to add...
I am now writing this on Saturday, 30th March and yesterday (Good Friday) Pam arrived back home by ambulance (via an ultra-short pause at MBH following the flight) and was in my care at 3pm. This was the scheduled time for one of Pam's 200ml hydration flushes and this particular one is not medicated. All went well although it was annoying that the input nozzle didn’t seem to be designed for the syringes I use for hydration. It was quite ‘loose’.
5pm came, and another (this time medicated) hydration flush was uneventful as was the 7pm medicated flush. But at 9pm when I gave Pam a 50ml pre-flush of Nexium anti-nausea, prior to her 9:30 PEG feed, the tube promptly blocked and no amount of effort would overcome the blockage. There was no point attempting to pump her nightly PEG feed because this blockage seemed to be meaning business – and so I rang 000 for an ambulance.
Pam was taken to Mildura Base Hospital (MBH) and they spent ages trying to unblock the tube. I reckoned that it was probably the Nexium, dissolved as it was to free the tiny time-release capsules and it was them, thought I, that had caused the blockage. I later learned some confirming input in that the gauge of this PEG is significantly less than the Stomach PEG that it replaced and the reason that it hadn’t blocked with Nexium prior to my doing it was that the hospital staff of both hospitals, were crushing the Nexium tablets as they did with every other tableted med. This may have avoided the potential blockage, but was a definite no-no according to the instructions written on the packet. (Hospital staff personnel are seemingly oblivious to instructions on tablet packs, probably because they only deal with the foils already taken from the packs, and a tablet is a tablet.) I have also discovered since beginning this paragraph the gauge of the blocked PEG is vastly smaller than the one it replaced i.e. the one that fell out.
The yellow tube is from the tube that fell out - simple single tube. The bluey-grey one (i.e. the one that blocked yesterday) is compound, but clearly not a tube-within-a-tube as was the stomach PEG. Here, the tiny hole is for the locking balloon and the larger of the two is for food flow. Compare this diameter with that of the yellow. No wonder it blocked, in hindsight.
This has me wondering about the new one fitted today. It's different in appearance, but this sort of a test is not appropriate ... yet.

It was getting late and the ambulance officers offered to take Pam home to bed rather than leave her on a trolley all night as the hospital had no bed space. So at 2:50am this morning, I put Pam to bed. The ambulance guys then recommended that I make an early booking (8am) so that they could get Pam back to the MBH at a reasonable time to either succeed with the unblocking or to Air Ambulance Pam back to Adelaide for a new PEG.
So I got up at 7:30 this morning, showered and shaved and
did what I was told.
Pam was in the ambulance at 8:30am and home again at 4pm –
seven and a half hours it took, to decide that the old PEG was stuffed and had
to be taken out. A new one subsequently fitted
(without Pam going to Adelaide) and eventually X-rayed to check for correct
insertion. The minutes (in bulk) ticked
by and at long last we were given the nod that the radiologist was satisfied
that the PEG tube was indeed inside Pam’s Jejunum.
Pam’s now happy and hydrated –
she had had nothing of the sort since 7pm the night before. As I write
this, Pam is watching ‘Packed to the Rafters’ which I recorded for her.
It’s occurred to me how
intuitively appropriate is the main title of this blog – but I fear that most
of the subsequent postings will be of a similar ilk.
I think the ambulance staff was surprised at the cleanliness of the colostomy and the approximate number of days for which that had been the case and so happily took Pam to the Base Hospital to see what could be done.
When I got there, I was quickly relieved to learn that if the food had indeed been emptying into Pam’s abdomen space, it would have been painful – but it wasn’t. An X-ray confirmed that the PEG tube was where it was supposed to be and that Pam was (merely) terribly constipated.
Pam was admitted to Ward 3 (room 17), stayed the night at the Base and I volunteered to look after many of the hydration flushes, four of them being medicated and also Pam’s overnight PEG feed. I get to bring her back home after lunch today, Sunday 7th.
When I got there, I was quickly relieved to learn that if the food had indeed been emptying into Pam’s abdomen space, it would have been painful – but it wasn’t. An X-ray confirmed that the PEG tube was where it was supposed to be and that Pam was (merely) terribly constipated.
Pam was admitted to Ward 3 (room 17), stayed the night at the Base and I volunteered to look after many of the hydration flushes, four of them being medicated and also Pam’s overnight PEG feed. I get to bring her back home after lunch today, Sunday 7th.
What’s next, I wonder?